Bisphosphonates vs. BHRT · the honest comparison
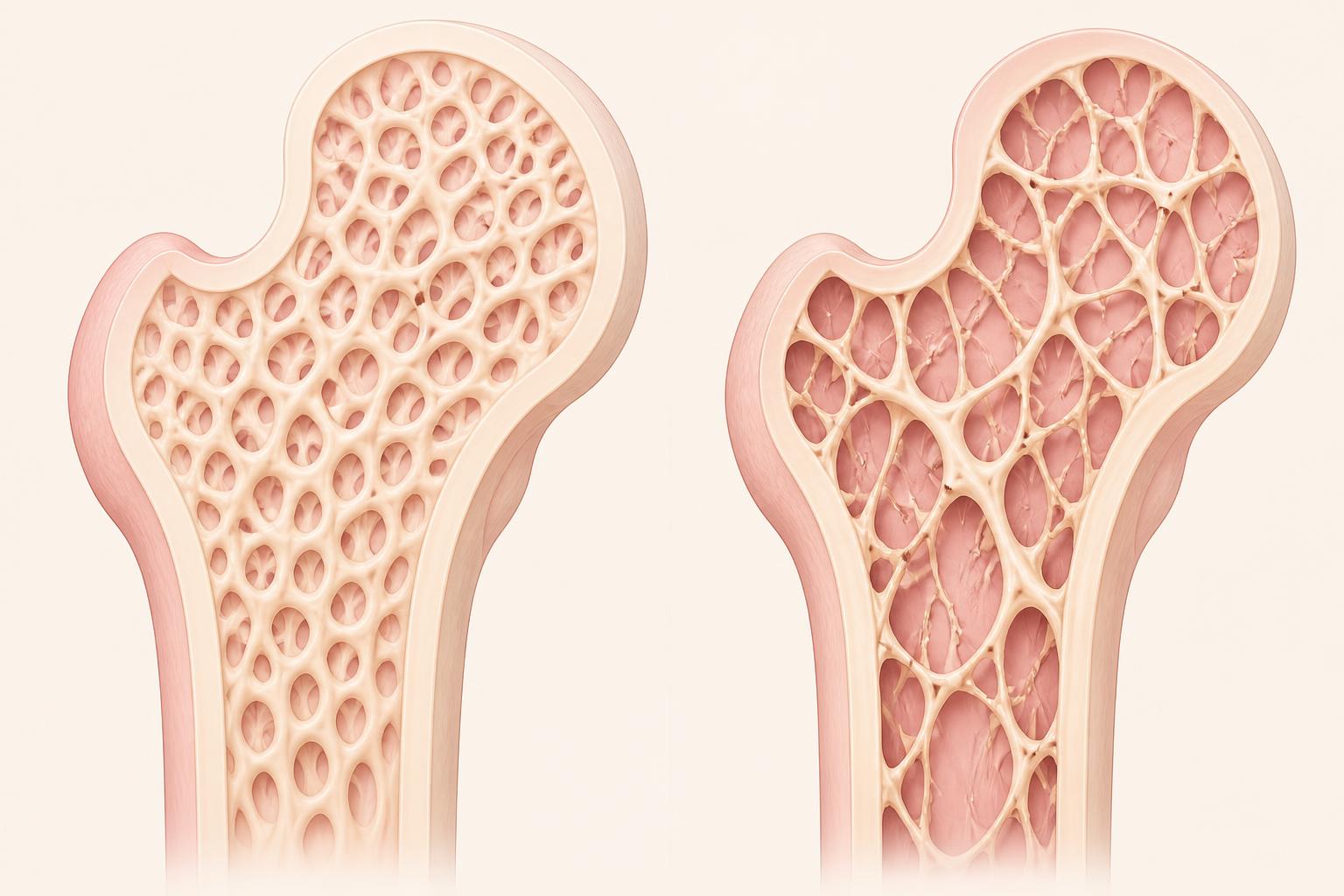
Estrogen keeps the bone bank from being robbed. Bisphosphonates put a lock on the vault.
Bisphosphonates aren't "evil" — but they aren't candy either. They can be lifesaving for the right patient. They are also overprescribed to women whose real issue is estrogen loss, low vitamin D, or untreated thyroid disease. The honest question isn't "do I have osteopenia?" — it's "what is my actual fracture risk?"
Bisphosphonates
Fosamax · Actonel · Boniva · Reclast
Slow down osteoclasts — the cells that break down bone. That reduces bone turnover and lowers fracture risk in patients who truly need it. Considered first-line for osteoporosis, fragility-fracture history, or high-FRAX osteopenia.
Upside
Proven fracture-risk reduction at the hip and spine.
Common risks
Reflux, esophagitis, nausea — oral forms need strict dosing (empty stomach, upright 30 min).
Rare but serious
Osteonecrosis of the jaw, atypical femur fractures — usually with longer use.
Reassess at
3–5 years of oral therapy, or after several IV doses — a real stop-and-think moment, not "forever."
BHRT / Menopausal hormone therapy
Estrogen — sometimes with progesterone
Restores some of the hormonal environment your bones evolved with. In the WHI trials, hormone therapy reduced osteoporotic fractures. For many menopausal women, it's a logical foundation when estrogen loss is part of why density dropped.
Upside
Prevents ongoing bone loss + treats hot flashes, sleep, mood, GU symptoms.
Best window
Under age 60 or within 10 years of menopause — when the risk-benefit math is most favorable.
Not enough alone
For established osteoporosis or prior fragility fracture, hormones may not be sufficient by themselves.
Personalized
Type, route, dose, history, breast and clotting risk all factor in — never one-size-fits-all.
Dr. Tammy's clinical take
"Some women need the estrogen. Some need the lock on the vault. Some need both. But nobody should be handed a prescription without knowing why."
For osteopenia with good estrogen, good D, no fragility fracture, and a low FRAX: lead with food-first calcium, protein, progressive resistance training, impact work, fall prevention, magnesium, vitamin K, thyroid + parathyroid evaluation, and a repeat DEXA in 1–2 years. For osteoporosis, a prior fragility fracture, a T-score below −2.5, or a high FRAX score: bisphosphonates (or anabolic agents) deserve a real, not fear-based, conversation — and BHRT may sit alongside them, not instead of them.